
[ad_1]
According to an article in Down to Earth, published in May 2026, there is an imminent need to recognise heat as a gendered climate disaster. Studies show that “women’s bodies respond differently to heat stress at a physiological level. Hormonal fluctuations, body composition, and metabolic rates all affect thermoregulation, making women more susceptible to dehydration, fatigue, and heat-related illness. Pregnant women face even greater risks… heat waves add to the challenges faced by already fragile maternal health systems”.
Heat-related discussions and their links with women’s health remain marginal in discussions around climate change; the idea that heat poses a special danger to women’s bodies has a surprisingly long history in India. However, most colonial environmental anxieties regarding heat and women’s bodies centred less on women themselves than on their reproductive capacity.
Over two centuries ago, tropical medicine and colonial administration brought the debilitating effects of heat into focus in public health discussions. Heat was rendered into a cause and a diagnosis as early as the 18th century when the East India Company encountered severe adversities, either because the sultry tropical climate itself was a survival challenge for the unacclamatised European bodies or due to health threats ranging from heat apoplexies to more deadly tropical diseases like cholera and malaria that were directly linked to the hot weather.
India was an epidemic-prone country, and before the discovery of “germs”, the “miasma theory” dictated that contagion was rooted in atmospheric elements. European physicians worried endlessly about the pestilential climate and the insanitary ways of “natives” that could wipe out large populations of Europeans without warning. John Pringle, Observations on the diseases of the army (first published in 1752), made extensive notes on the diseases occasioned by heat. He wrote:
…the heats have been sometimes so great as to prove the more immediate cause of particular disorders; as when centinels were placed without cover, or frequent reliefs, in a scorching sun; or when the troops marched, or were exercised in the heat of the day; or when the men imprudently lay down and fell asleep in the sun; all which circumstances were apt to bring on distempers. varying according to the season. In the beginning of summer, such errors produce inflammatory fevers; and at the end of it, or in the beginning of autumn, a remitting fever, or a dysentery.
Extreme heat had hitherto never concerned European medical authorities, but as the British imperial ambitions expanded, it became identified as a major impediment in military and administrative affairs. As medical science progressed, the harmful effects of heat figured prominently in mainstream medical discourses, as a causal factor for numerous afflictions and aberrations in the human body and mind, ranging from indolence to risky sexual behaviours.
This, however, needs to be understood keeping in mind the colonialists’ tendency to imagine India and its environment and topography as insalubrious and hostile to Europeans. Historians like Mark Harrison have discussed how the uniqueness of the Indian environment and its maladies necessitated a reappraisal of European medical knowledge in light of the new circumstances. According to Harrison, there were two main questions before the Europeans: whether they would be able to adapt to their new environment, and if they would be able to draw on Indian indigenous methods of healing to create a new branch of tropical therapeutics to help them survive in the colony.
As British women began to travel and migrate to the colonial outposts in increasing numbers in the 19th century, the medical community scrambled to study the effects of the tropical environment on European women’s bodies and minds as well. The presence of women on the colonial frontiers signalled the expansion of the Empire in the east. However, European female bodies were already “fragile”, and the extreme tropical climate that had already humbled the male members of the European race became identified as a causal factor for uterine complications. Heat, then, could potentially jeopardise the future of empire-making by hampering female reproductive health. Colonial physician Edward Tilt wrote in Influence of India on the health of British women, and on the prevention of uterine affections (1868):
…as tropical climates produce uterine inflammation, because habitually intense heat disturbs menstruation in those who were not born under tropical influences, so our countrywomen, when transplanted into India, become more liable to inflammation of the womb, as a result of pregnancy, abortion, and parturition, than if they had remained in England.
At that time, the focus on heat in female-health matters was indeed quite novel for the Europeans, who were otherwise concerned with diseases that emerged from low temperatures, such as tuberculosis, which the Victorians widely romanticised and linked with feminine frailty. Medical authorities frequently blamed the “chills” as the cause for a wide variety of female-specific ailments. Menstruation, for instance, was believed to be a way through which the body was purged of impure blood through a monthly cleansing process that maintained health. This is because even in the 19th century, European medicine contained traces of Hippocrates’ humoral theory, which dictated that the body needed to maintain the right balance of blood, phlegm, yellow bile and black bile. If a woman got cold, her blood vessels were thought to constrict or “freeze,” stopping the flow. Victorian obstetricians and gynaecologists warned that activities such as bathing in cold water, washing clothes, or working in damp conditions would halt the menstrual flow.
Paradoxically, in tropical medicine, heat was not only believed to cause uterine disorders but also caused prolonged suffering due to disturbances in the female reproductive system, bringing on the “chills” due to the constant perspiration. The infamous Indian climate, therefore, required a new subsection of gynaecological and obstetrical practice, which could study, diagnose and treat heat-related female health ailments. Physicians like Tilt developed scientific strategies to allow the European female reproductive system to adapt to the eastern climate to facilitate the imperial project through safe and easy childbearing.
The health of the womb was necessary as medical complications could hinder the primary colonial project, which required the propagation of the British race in India. Indeed, various medical treatises and manuals repeatedly asked whether European women could conceive, carry, and raise healthy children in the Indian subcontinent, effectively bringing heat to the forefront of medical discourse. By the mid-nineteenth century, British women travelling to India could refer to a growing body of medical literature, including a variety of popular domestic guides, self-help books on female health and hygiene in the tropics, and maternal advice books, which were useful, given that the medical advice otherwise known to them was only applicable in a temperate climate.
Some of the methods recommended to women for their gynaecological wellbeing could be drastic, as well as what we would now consider bizarre. Tilt, for instance, recommended regular cold water vaginal douches administered with specially designed syphon syringes made from a vulcanised India-rubber. According to Tilt, such practices could prevent inflammation, regulate excessive secretions, and help European women “prolong their residence in a hot climate”. Although this medical advice is obsolete, what strikes as particularly contemporary are the attempts to connect heat exposure to preterm birth, pregnancy complications, maternal complications and negative reproductive outcomes.
Apart from such classic Victorian therapeutics, there were other survival strategies the British adopted to adapt to the climate: Colonial residences, unlike charming English cottages, had their own peculiar architecture, with verandahs wrapped around the entire periphery of the house, and tall louvred windows that allowed the breeze through, although during the summer months, hot winds called “loo” blew throughout the day, and the interiors of the bungalows could become extremely suffocating
The most common machinery to deal with the stuffiness was the manual punkah system that was operated by the “punkahwallas” or punkah coolies. Historian Arun Kumar wrote in a 2022 article published in Scroll that the punkahwallas were cheap labourers who were “natives” and were kept awake all night so that their British masters could sleep, with breaks in early morning. They would often be rudely awakened by the sahibs if they fell asleep on the job and were punished for their truancy. The wealthy white families had punkahs over their beds, dining tables, bathtubs and so on.

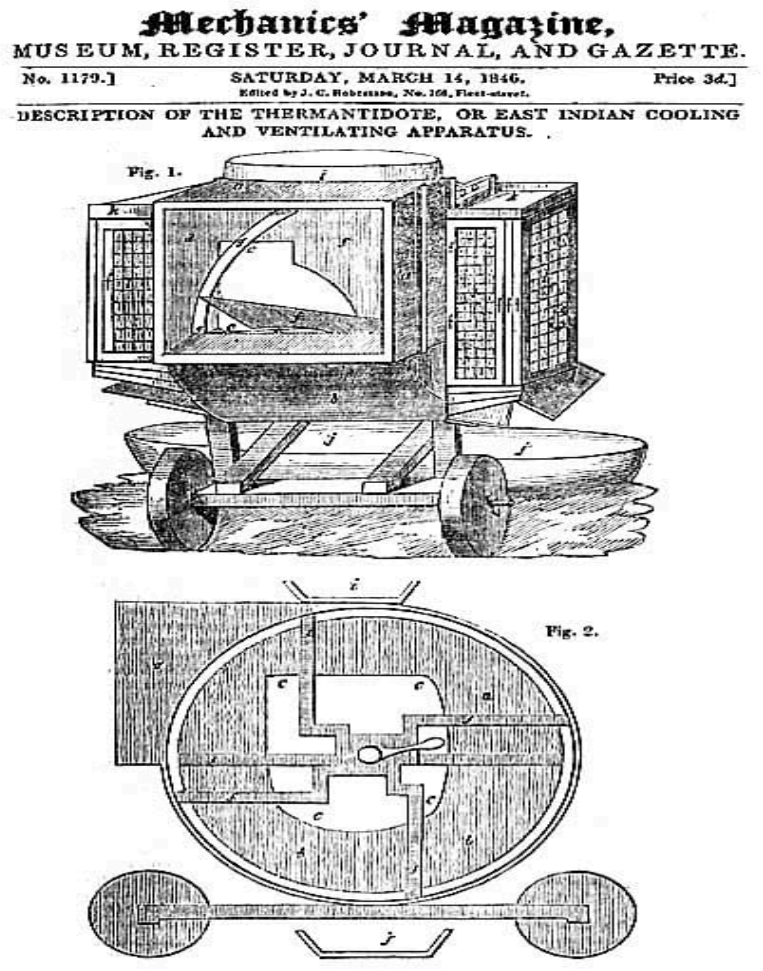
Those who could afford it owned the thermantidote – an ingenious household cooling contraption that the traveller and self-proclaimed ethnographer, Fanny Parkes, wrote about in Wanderings of a Pilgrim in Search of the Picturesque (1850):
The thermantidote is a structure awful to behold… an enormous machine for forcing cool air into the house; it is made of amra (mango wood), or sakoo: the wheels and axle are of iron, In height, is is about seven feet, in breadth four or five, and some nine or ten or 12 feet in length… in the interior, four large fans are affixed… is turned round by two men on the outside
Clothing was another cause for concern. Far from the silks and wool, the sahibs and memsahibs wore muslin and other breathable fabrics. British women tried to hold onto Victorian fashion, but practical guides recommended otherwise. Medical advice could, however, be contradictory. Mary Scharlieb, the pioneering British gynaecologist who wrote A Woman’s Words to Women: On the Care of Their Health in England and India (1895), suggested wearing light silk and woollen underclothing to avoid the chills caused by perspiration.
The most preferred method of avoiding the heat was evacuation to cooler climes. The seriousness of the matter can be understood by the Viceroy, Sir John Lawrence’s decision for the administrative heads to operate from Shimla in the summer months, in the year 1864, when it was made the British summer capital. Shimla’s climate resembled European weather, and it already had small hamlets since the beginning of the 19th century. Starting that year, a large body of British officials, ranging from civil servants to thousands of imperial clerks, went between Calcutta and Shimla, normally for March/April through October. Much later, the Kalka–Shimla railway made the journey of 1600 kilometres less arduous. In the 1870s, Robert Bulwer-Lytton, the Viceroy at the time, planned the town and laid the foundation for the Viceregal Lodge (which houses the Indian Institute of Advanced Studies today).
The physician Tilt himself emphasised the merits of British women migrating to the hills in the summer. Many had temporary residences in the hill towns of the Himalayas in northern India or the Nilgiris in the south, or rented bungalows or inns for the season in any of the popular hill stations, where they stayed with or without their husbands. Their sojourns in hill stations such as Mussoorie and Shimla figure prominently in the wide corpus of literature created by them about their life and travels in India. Mainly for this, they are often villainised in popular culture for their selfishness in forsaking their husbands, who would be slogging in the plains. It didn’t help their case that most hill stations were social hubs where leisure, gossip, and entertainment were the prime engagement. Several tantalising tales of their summer escapades in the hills, including clandestine meetings and illicit affairs, emerged from these long stays in the hills.
However, for the memsahibs (British women), bad repute due to neglect of conjugal duties was one challenge greater than the heat during Indian summers. Those who chose to stay in the plains struggled with the heat and humidity day and night. Monica Campbell Martin, who came to India with her husband, Peter Martin, in the year 1923, wrote that no woman could look well in the weather: “You long to take off your skin and sit in your bones. You are a slab of melted butter.”
The only respite was the cool evening when they played light sports, because these were the only games that could be played after sundown, in the small window between dusk and twilight. Women passed the time somehow until evening, when they ventured out for a walk around the bungalows or played “hot-weather badminton”.
However, there were restrictions in this too: Victorian physicians had strict medical advice for women in the Raj, and often advised against any exertion or vigorous exercise. Birch wrote:
In the heat of the plains, all that is needed is gentle exercise once or twice a day, and a life lived out of doors. Some women are better without any games or dancing… all exercise should stop short of inducing a fatigued feeling or exhaustion, since this means a lowering of the vitality and renders the system more liable to chills and malarial poison… bicycling should only be indulged in by the young and strong, in moderation. A woman should sit well back on the gluteal region, not on the perineum in front, and lean slightly forward on the saddle.
Today, heat is quickly becoming a global health concern as weather-related deaths and illnesses are currently on the rise. Between 2000 and 2019, studies show approximately 4,89,000 heat-related deaths occur each year, with 45% of these in Asia and 36% in Europe. In Europe alone in the summer of 2022, an estimated 61,672 heat-related excess deaths occurred. The global climate crisis makes the situation increasingly perilous, and the negative consequences on health can be avoided or tackled with policy and medical interventions.
Currently, the preventable nature of heat-related health concerns is precisely why the rising mortality rates are even more concerning. While vulnerability to heat is contingent upon various physiological as well as exposure factors, women’s health seems to be at particular risk. In a 2025 study published in The Lancet, it was reported that a systematic review and meta-analysis found that for every 1-degree increase in heat exposure, there was a 4% increase in the odds of preterm birth. Another 2025 study attempts to unravel how heat-related health effects intersect with housing conditions and occupational risks, to inform policy recommendations.
Victorian gynaecologists misunderstood much about female health conditions; yet, they were among the first to link prolonged heat exposure to reproductive health. Almost two centuries later, as global temperatures rise, the question has emerged with alarming force. The Victorians at least teach us that a lot more attention is needed in this domain of medicine, and that heat is indeed gendered. Moving forward, the health implications of heat on women, women-centric climate resilience, and gender in health adaptation need greater focus.
These histories are explored in greater detail in Ipshita Nath’s forthcoming book In Sickness and in Death: How Faith, Medicine and Race Shaped British India.
[ad_2]
Source link